Add / Edit Benefit Plans
Click the Benefit Plan category button on the Scenario page.
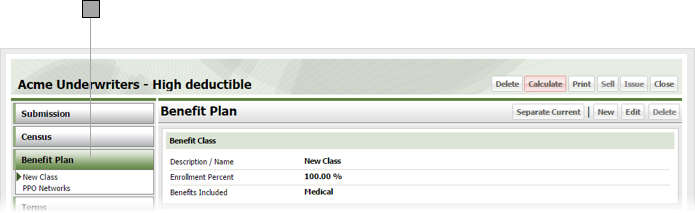
Do one of the following:
- Add a benefit plan to the scenario by clicking New.
- Edit an existing benefit plan in the scenario by selecting it from list of plans under the Benefit Plan category button, then click Edit.
ESL displays either a blank Benefit Plan window, or a Benefit Plan window containing the information for the selected plan.
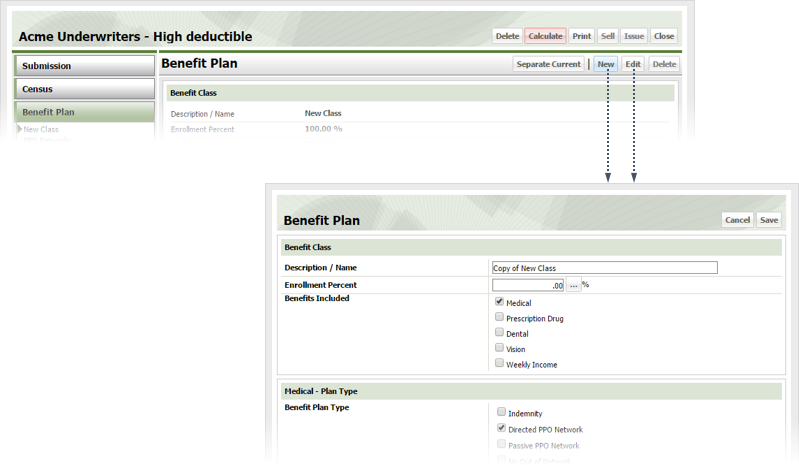
Give the plan a name in the Description / Name field.
Click the button to the right of the Enrollment Percent field to display the Utilization window.
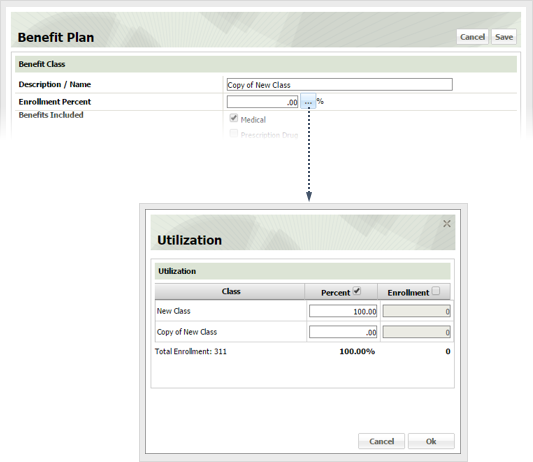
Specify plan utilization as follows, then click OK.
Check the box by each benefit included in the plan. Checking a box causes its corresponding section in the benefit plan window to appear.
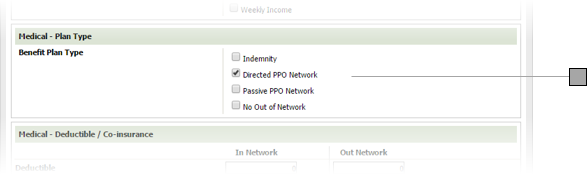
If the plan includes Medical, check the appropriate Benefit Plan Type box.
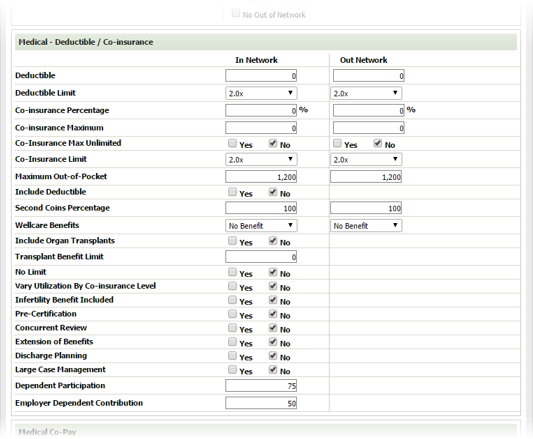
If the plan includes Medical, specify deductible and co-insurance information as follows.
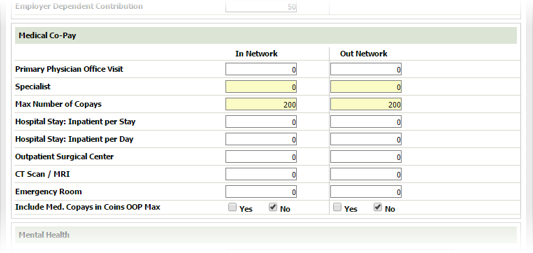
If the plan includes Medical, specify co-pay information as follows
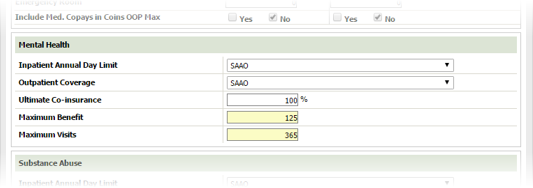
If the plan includes Medical, specify mental health coverage as follows
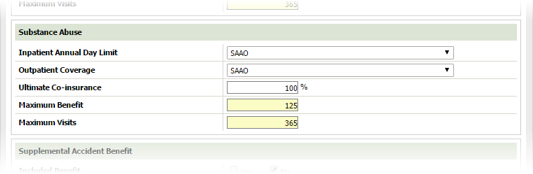
If the plan includes Medical, specify substance abuse coverage as follows
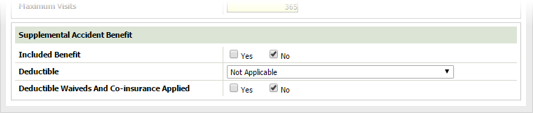
If the plan includes Medical, specify supplemental accident benefit coverage as follows
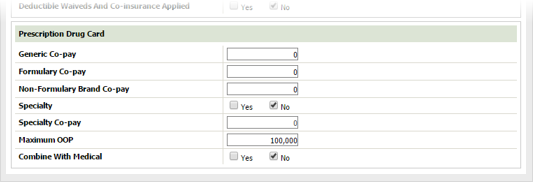
If the plan includes prescription coverage, specify coverage details as follows
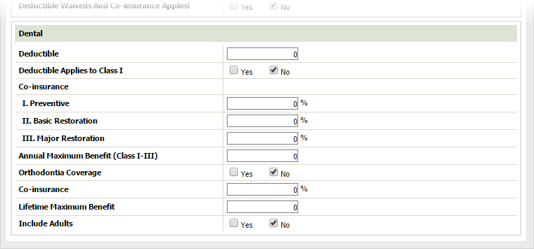
If the plan includes dental coverage, specify coverage details as follows
Click Save.